 Laura Brooks
Categories: Uncategorized
8084
Ultivue announces launch of new configurable multiplex spatial panels at the Society for Immunotherapy of Cancer 2023 meeting
Adrian Arechiga
Categories: Uncategorized
6718
SITC recap 2022
Laura Brooks
Categories: Uncategorized
8084
Ultivue announces launch of new configurable multiplex spatial panels at the Society for Immunotherapy of Cancer 2023 meeting
Adrian Arechiga
Categories: Uncategorized
6718
SITC recap 2022
It was a record year of attendance at this year’s 37th annual SITC meeting. Whether reflective of waning new Covid cases from a peak in late January 2022, a new location, or merely the appetite to meet up with colleagues, check out new technologies or be part of important scientific discussions-Boston SITC had it all. As one of the top research cities in the world, over 1,000 biotech companies, often early start-ups, call the Greater Boston area home. Several factors play into this dominance including its proximity to Harvard Medical School, the Massachusetts Institute of Technology (MIT), Dana-Faber Cancer Institute, Massachusetts General Hospital, and other leading academic institutions. This collaborative scientific mindset encouraging rapid communication and collaboration was very much present at SITC2022.
While a better understanding of cancer immunobiology has increased dramatically in recent years, leading to the successful development of novel immune-based treatment options, unfortunately, only around 20 to 30 percent of solid cancer patients given immunotherapies go into long-term remission. The goal at SITC therefore “aims to make cancer immunotherapy a standard of care and the word “cure” a reality for cancer patients everywhere”. The 3-day meeting and pre-meeting workshops offered valuable scientific educational sessions with key opinion leaders and the latest cutting-edge research summarized in talks and over 1800 posters.
Spatial biology and novel biomarker discovery was front and center at the meeting with several dedicated sessions addressing the complexity of the immune network and tumor microenvironment. Of note was the number of techniques using various high-dimensional methods for exploration of both tissue and blood samples at the genomic, transcriptomic, proteomic, and even microbiome level, in relation to overall treatment response and adverse side effects.
A particularly impressive example of combining methods to achieve a novel understanding of immune response in the tumor microenvironment came from research out of the Sharma lab at MD Anderson (1). With a talk entitled “High-dimensional analyses of intratumoral myeloid cells highlights presence of distinct myeloid cell phenotypes in immune checkpoint-sensitive and resistant tumors”, they presented a comparative analysis of intratumoral myeloid cell subsets to identify the phenotype of immunosuppressive myeloid cells and to identify potential combination strategies to improve immune checkpoint blockade therapy (ICT). Myeloid cells in orthotopic mouse models of ICT responsive (B16F10 melanoma) and ICT non-responsive (MT4 pancreatic) tumors pre- and post-ICT were analyzed via single cell RNA sequencing and multiplexed IHC approaches. scRNAseq of tumor and stromal cells from MT4 and human pancreatic tumors indicated that cancer associated fibroblasts (CAFs) from pancreatic tumors express elevated levels of TNF Stimulating Gene 6 (TSG-6), an anti-inflammatory molecule, that inhibits a pro-inflammatory phenotype and promotes an anti-inflammatory phenotype in myeloid cells. Blocking TSG-6 with monoclonal antibody improved survival and response to ICT in mice with pancreatic tumors by decreasing immunosuppressive myeloid cells and increasing abundance of CD8 T cells. The authors concluded that overall, the data supported a model in which TSG-6, expressed at high levels by CAFs, promotes an immunosuppressive phenotype in myeloid cells in the tumor.
Additional talks addressing the presence and density of CD8+ cells and other immune cell types were high on the agenda. This is especially important as we can now start to appreciate that the spatial pattern analysis of tumors and specific cell co-localization could provide detailed information on overall cancer prognosis. Increasingly, data supports the value of spatial measurement of T cell infiltrates as a novel, robust tumor-immune biomarker. In a talk entitled, “CD8+FoxP3+ cells represent early, effector T-cells and predict outcomes in patients with resectable non-small cell lung carcinoma (NSCLC) receiving neoadjuvant anti-PD-1-based therapy” work from the Cottrell lab at Queens University, Ontario presented a study to identify biomarkers of therapeutic response in patients with non-small cell lung carcinoma (NSCLC) receiving neoadjuvant anti-PD-1 therapy (2). Pre-treatment tumor specimens from patients in the clinical trial of neoadjuvant nivolumab +/- ipilimumab were stained with a 6-marker multiplexed immunofluorescence (mIF) panel for PD-1, PD-L1, CD8, CD163, FoxP3, and cytokeratin. Densities of immune cell populations were analyzed, and the presence of CD8+ FoxP3+ cells correlated with response to neoadjuvant immune checkpoint blockade (ICB). Importantly, the presence of CD8+ FoxP3+ cells were also associated with improved event free survival and overall survival.
The highly interactive two-day poster sessions were packed, encompassing over 1800 novel research findings. Many of the studies also included spatial work, indicating the importance not just of the technologies used to address the presence of specific markers within the tumor microenvironment, but also the image and AI tools used to address cell interactions and proximity. Work from the McKee lab at the Hôpitaux Universitaires de Genève in Switzerland using a 12-marker mIF panel addressed the important differences between MSI (microsatellite unstable) and MSS (microsatellite stable) colorectal cancer biopsies (3). By characterizing the phenotype of the T-lymphocyte population and their localization using cell neighborhoods (CN), analysis identified elements, such as epithelial cells and tertiary lymphoid structures (TLS), that the authors concluded may help to define both the prognosis of tumors and the possibility of a response to immune checkpoint therapy. A number of posters focused on the presence of TLS’s which is known to correlate with a favorable prognosis in many types of cancer. In their poster entitled “Maturation and abundance of tertiary lymphoid structures are associated with the efficacy of neoadjuvant chemoimmunotherapy in resectable non-small cell lung cancer” the Yue group at Tianjin Medical University Cancer Institute and Hospital, Tianjin, China investigated TLS maturation and abundance in resectable NSCLC receiving neoadjuvant treatments (4). The TLS in tumor tissues was detected by mIF and the differences in TLS maturation and abundance among different treatment groups were analyzed, as well as the relationship with pathological response and prognosis of patients. Multiplex analysis showed an increased infiltration of CD8+T cell and decreased infiltration of M1 and M2 macrophages after neoadjuvant chemoimmunotherapy treatment in patients achieving response. Overall, the results demonstrated that TLS maturation may be a potential mechanism of action of neoadjuvant chemoimmunotherapy in resectable NSCLC.
It’s clear based on all the interactions at SITC2022 that spatial biology and the utility of mIF is enhancing the depth of our understanding of disease mechanisms and helping us interpret what cellular changes might be clinically meaningful. To allow deeper discovery of biological insights, the next steps to fully utilize the power of spatial analysis will need to ensure harmonization with the computational methods and pipelines for data analysis. All told, there’s a lot to look forward to in this field in 2023.
Want to learn how spatial phenomics can help guide some of your research, https://ultivue.com/spatial-phenomics/. Please reach out to one of our experts today, https://ultivue.com/contact/
References
1. https://jitc.bmj.com/content/10/Suppl_2/A528
2. https://jitc.bmj.com/content/10/Suppl_2/A63
3. https://jitc.bmj.com/content/10/Suppl_2/A1321
4. https://jitc.bmj.com/content/10/11/e005531
 Eva
Categories: Uncategorized Tags: Point of VUE
6535
Living in a Spatial World Q&A, Part 2
Eva
Categories: Uncategorized Tags: Point of VUE
6535
Living in a Spatial World Q&A, Part 2
GEN: Typically, image analysis tools are greatly influenced by inconsistent staining results and even different techniques used for multiplexing. How does the software used by OracleBio account for inter- and intra-run variability in staining quality?
Lorcan. To be honest, we do see staining variability in some sample sets, especially in complex tissues from large clinical sample sets of images. That staining variance can come in through some pre-analytical steps that can come from the tissue, assay etc. So, when we get the images for image analysis, yes, there’s a number of things that may already have happened at the pre-analytical stage that we can’t solve, but we can solve some levels of variance within the algorithms we’ve developed. We do this using AI deep learning approaches in our algorithm development.
For example, if we’re looking at something like tumor stroma segmentation with a tissue classifier and we’re using the cytokeratin layer and DAPI to train the deep learning algorithm, then if we have, say, 100 images in the study and we want to use 20 of those images to train an algorithm, we will export the actual mean intensity for the cytokeratin channel from each of the hundred images. We will look at each of the 100 images and look for those images where there is quite a high mean intensity, which means there’s more intense staining. For the images that are low intensity or have low levels of staining present, we will make sure that they’re both included in the training image set for the deep learning algorithms so that we’re exposing the algorithm to this range of variance that we may see in a sample set.
From a cell detection perspective, a very similar approach is taken where if we’re detecting e.g., CD68 cells or CD3 cells in an algorithm specifically as a top line lineage, we will look across the whole image set during the algorithm development stage. We will identify those images where the staining is weaker, or the staining is stronger based on the mean intensity across the tumor microenvironment, and we’ll make sure that those images are included. Of course, a mean intensity can tell you two things: It can tell you that generally all the cells are staining low, or it may tell you that there’s a bunch of cells there that are staining really well, but there’s just less of them, so we do need to take that into context.
In summary, I would say that by incorporating a deep learning approach into the algorithm development, we are moving away from a more standard threshold approach, where we choose a single threshold and then try and apply that to a large set of images where we may see variance. Instead, by using deep learning, we are starting to move more to an adaptive threshold approach. I think with this it does allow us to manage some of the variance that we see in these types of images. We’re moving from single chromogenic, where there was only one or two channels of interest and DAB staining, to now four, 8, 12 plex and higher where there’s multiple channels with variance in each channel. So yes, I think AI deep learning has been a big help in helping manage some of that variance.
GEN: Will we ever be able to come to a consensus on best practices for AI driven digital pathology? Or is this strictly tumor or tissue dependent?
Lorcan: Yes, I think when we talk about AI and digital pathology, it’s such a dynamic space now and there is so much ongoing development in the assays that we are seeing coming through. As I said in my presentation, this comes from all the updated scanning capabilities to the available information in the images and the strength and power of these neural networks.
But let’s not forget that the abilities of these neural networks may be very different in a couple of years’ time, so we are dealing with a very dynamic, moving landscape. With that in mind, to pin down best practices can be quite challenging. To date the algorithms developed are very much focused around answering specific questions, e.g., dealing with segmentation of tumor-stroma and identification of cells.
I think as our knowledge and use of AI develops and as we move to identifying more biological or spatial signatures from clinical sets, and that information moves more towards a diagnostic endpoint or gets closer to specific use with the patient, then I do think best practices will really come much sharper into focus. And regarding things like how do we standardize the development of these apps? I think at the moment it’s just a really dynamic area. Certainly, this is something that needs to be established to get us closer to the patient with these services and technologies.
GEN For the deep learning algorithm with additional H&E layer, is that a serial section or the same exact section used for the multiplex IF?
The images that we get from Ultivue have the RGB single channels built into the TIFF image, and they can be switched on to create the H&E images which is a real benefit not just to us, but as I said in my presentation, also to pathologists who are working on these image
Lorcan Sherry
CSO & Co-founder of OracleBio
Lorcan: Short answer, yes. It’s the same section, and from a digital pathology image analysis perspective, it is so valuable to have that H&E built into the same section. This is something that Ultivue have really taken on and tried to standardize in how they present their images for subsequent in-depth image analysis. And bear in mind, while you can certainly take serial sections and you can certainly align serial sections, you’re really not able to completely align the data. This may be okay for tissue classification purposes. But if you’re looking for specific cell identification with H&E or are trying to support algorithm development from a cell detection perspective with the H&E component of the image, it does become more challenging when you’re trying to use a serial section co-registered to a multiplex image. The images that we get from Ultivue have the RGB single channels built into the TIFF image, and they can be switched on to create the H&E images which is a real benefit not just to us, but as I said in my presentation, also to pathologists who are working on these images.
Gen: How do you analyze high plex images, say 30 to 40 markers? Do you use manual thresholding for each marker?
Lorcan: Obviously, these approaches can be quite complex with respect to high plex assays, especially going up to 30 or 40. I think, with how we use deep learning algorithms at the minute, it’s also to do with the number of channels that you can use within the neural network and that can be used to train a neural network.
A lot of neural networks are trained on traditional RGB images, which restricts them to three channels for deep learning purposes. We can certainly use AI as an approach for some of those markers around, say, accurate segmentation of cells, using nuclear markers, or T cell or macrophage lineage markers. Then we can use a manual thresholding approach for several of the other markers. You can either take all these efforts and try to build it all out into one algorithm, or the other option is that you use several different algorithms on a high plex image so that you specifically develop AI maybe for three or four markers of interest. You create data for those three or four markers, and you set up a number of algorithms that are AI based. Then you export the data for each of these algorithms and combine it to do post-processing for spatial analysis.
So, there’s different ways to do this, and it really depends on how much you want to frontload different algorithm approaches and try and incorporate an adaptive approach. Alternatively, you may want to combine AI with manual thresholds. For us as a company and what we provide as a service, we must also take into consideration overall time and turnaround time, as well as cost. Ultimately, there will be components where we will potentially combine, say, AI with manual approaches for large cohorts and high plex image analysis.
Gen: What is the limitation of using open-source software compared with licensed image analysis software? Can the data be reliable?
Lorcan: Yes, that’s a good question. I can only really speak from our perspective as a contract research organization. We have traditionally used commercially available software. We use Visiopharm and Indica Labs Halo. We have service contracts with those companies which really gives us confidence that the software is getting developed in the correct way. It’s validated by them. Any potential bugs that may arise we can turn over to their respective service teams to get those bugs fixed and get back on track quickly. So the end product is good, and ultimately we have confidence that the data coming out of the software is going to be accurate and robust, in line with our client’s expectations.
On the flip side of the coin, we are in such a dynamic area that we do know there is never going to be one software that will answer or solve all the questions. I did mention that we do some Python scripting and MATLAB capabilities in-house, and I know there are a number of open-source software that are being extensively used from a research perspective to really drive forward the understanding of spatial biology. I would say to people, yes, you absolutely can use those. Specifically, if you bring them internally, you can do some level of validation, you’re comfortable and confident that they are acting accordingly, and your data is robust, then these contributions may help move data forward and help identify spatial signatures.
Ultimately, I think it’s a question that is probably quite specific to whatever individual and their circumstances that are used. I’m not going to say you shouldn’t use open-source software by any stretch, but from a commercial perspective, it’s important for us to also have the reliability of service arms behind us that we can rely on to help us with any issues.
If you have any questions, or would like more information on some of the topics discussed during this Q&A session, please look through our scientific content available in our resource center, https://ultivue.com/resource-center
hafadmin Categories: Uncategorized Tags: digital pathology, multiplex image analysis, Points of VUE, tumor microenvironment 6490 Living in a Spatial World Q&A, Part 1GEN: If I were to design my own panel for immunofluorescence, what are the main considerations, given everything you’ve suggested during the webinar for validation?
Angela: There are several things one needs to think about when you build a new panel for multiplexed immunofluorescence. You need to consider the abundance of the targets to be able to combine that target with the right fluorescence channel. Further, the use of good quality primary antibodies is especially important, particularly to assess their performance in chromogenic DAB, which is still the gold standard for a single plex assay before moving into building a multiplexed panel.
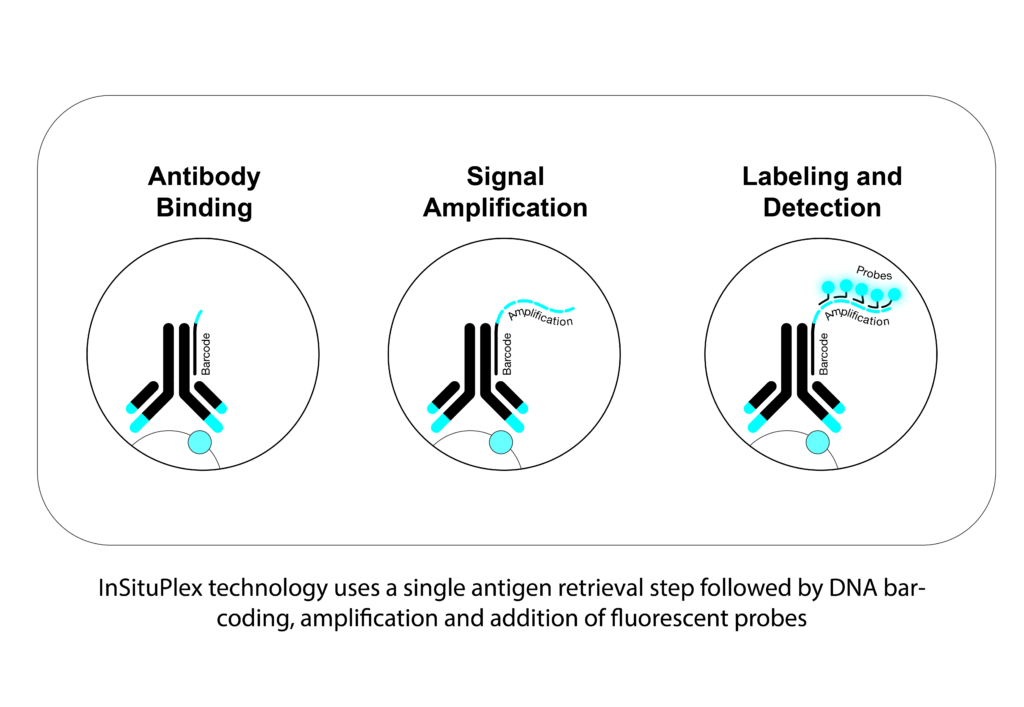
With InSituPlex® (ISP) technology you have fewer things that you need to consider as far as optimization and with that comes less variability because the workflow is pretty simple. For example, the end user won’t have issues with optimizing the concentration and optimal combination of an antibody. We don’t have a secondary antibody in the workflow, so this is also something researchers shouldn’t think about. And on top of that, because we deliberately use fluorescent channels that are spectrally distinct, you also don’t need to balance your signal. Another benefit of our technology is that we can amplify all the targets of interest at the same time, especially important for some weak signals.
GEN: Can you comment on what the best controls are for a multiplexed assay? Most companies use tonsil sample as the positive control, but is this really optimal?
Angela: Well, I would say it all depends on the type of targets you want to develop. If the target is well expressed in tonsil, that is a good starting point. At Ultivue, we always like to test the best conditions in the development of an assay, so we typically use control samples like tonsil and, where appropriate, on the actual tissue types that the study is going to be run on. Now that being said, when you are developing a target, it might not be expressed necessarily in tonsil. So ultimately what is important, is to use the appropriate tissue sample that expresses a good amount and a good level of the target of interest so that you can really identify the best conditions that would pick up low suppressors as well as high expressors of that target.
GEN: Is your H&E staining and multiplex IF used on the same slide?
What we do at Ultivue is perform multiplex IF as a first step, then we perform the H&E. This is not a virtual H&E, but instead the classically used H&E on the same exact tissue section.
Angela Vasaturo
Associate Director Scientific Affairs
Angela: The short answer is yes. Usually when we perform multiplex IF, we work on tissue paraffin embedded blocks. As far as a routine practice, once that’s performed, you’ll always have to have an additional H&E stained section from the block. With different sections, that H&E may not be truly representative of the actual tissue. In our case, it’s good practice to have the H&E from a block just to assess the quality in terms of fixation. But bear in mind, it’s critical to use the same section for the reasons that Lorcan explained for subsequent image analysis. So, what we do at Ultivue is perform multiplex IF as a first step, then we perform the H&E. This is not a virtual H&E, but instead the classically used H&E on the same exact tissue section.
GEN: Did you mention what kind of tissue preprocessing is required? Paraffin or OCT embedding?
Angela: We work with paraffin embedded samples. This doesn’t mean that the technology couldn’t be applicable to frozen samples, it’s just something that we haven’t wholly tested at this time because we focus mainly on clinical trials where paraffin embedded samples are most commonly used. With some additional steps for fixation, the technology could however be applicable to frozen (OCT) samples. But again, we haven’t tested that internally.
GEN: Angela, you mentioned there is 20% variability in the inter-, intra-day staining on the entire tissue section. While this is not a large difference maybe for known cell types, what about this variation in respect to rare unknown cell type combinations? Will this not impact further analysis downstream?
Angela: I would say that would be a little bit more difficult to evaluate on extremely rare phenotypes, and I think this is also the reason we use positive controls to evaluate the assay itself. Now, the biological variability is different than the intrinsic variability of the assay and although we are looking at the variability of the multiplex IF, we already take into consideration that 20% max of variability. There is also the component that comes from the instruments, for example, the autostainer, as well as the contribution of variance that comes from the image analysis. So, all of it is intricately linked and ultimately it is hard to really evaluate the true variability of any single component or reagent associated with multiplex IF.
Now that said, I think we have a lot to learn about those rare phenotypes. With the tools that we have for quantitative analysis, I think we are better placed today to really identify even pretty rare phenotypes by the unbiased way we look at the images. We are not pre-defining known phenotypes when you see the analysis; we really look at the single positive markers and then we combine those single positives to look at how many cells express multiples of the targets that are in the assay.
Lorcan: Yes, I agree, and I can add to that. When we talk about multiplex assays, we go from 4, 8 to 12 plex. The number of potential phenotypes that can be generated start to multiply quite substantially, and when you think about rarer phenotypes and maybe those that are not so obvious, it can be very difficult to validate and look at the variability for every single individual phenotype in something like an eight plex.
We’ve worked with Ultivue to address variance across sections that have been stained on different autostainers on different days, so what do we actually quantify? Well, we quantify every single channel for staining and how many positive cells are present for that particular marker within fields of view on sections. So, if you have an eight plex that will be 8 different readouts and that variance will be looked at, but we will also choose four or five of some of the main combined phenotypes, e.g. CD3, CD8, tumor PD-L1, and we will also count those as a phenotype manually and compare with the specific image analysis readout. All told we’ve at least got some reassurance that the variances are within the required parameters.
GEN: We have time for one last question. I think this is going to go to Angela. I’m going to combine two questions here, as I think the answers are probably short, but they’re also important. One of them, which I think is an interesting question, says the current spatial profiling is protein based, have you ever considered gene or RNA profiling based algorithms to do digital pathology? And then in connection with that, another audience member asked about limitation in terms of markers, they want to know what’s the max number of markers that can be used in multiplexing?
Angela: I think Lorcan can also help me a little bit on the digital pathology side with RNA, because he has more experience than I do. So while at Ultivue we look at proteins, there are also tools to look at RNA and actually we just presented a poster at AACR 2022 wherein we combined on the same section protein and RNA. Why would you choose one or the other if you can have both? I would be as provocative as I can be with this question.
And then the second part was the limitation in terms of number of targets, right? I think it depends on how we look at the field. At Ultivue, we currently have the maximum of 12 markers that one can choose from either our fixed off-the-shelf kits or our expansive U-VUE menu. It’s more like a choice in the sense that there are multiple companies that work in the digital and in the translational space, but also in the discovery space. When you are approaching things in a discovery way, then you need a lot of markers because this is where you need to generate your hypothesis. The more markers you can have, the better you can shape your hypothesis. Once you have done that and you need to validate your findings, you then want to reduce complexity. You wouldn’t want to go for 20-40 markers. In our experience, when you start from 12, or even eight, you have a good number of markers contributing to a very high number of phenotypes that you can identify and multiple hypotheses that you can validate at the same time.
We would suggest to researchers to initiate their studies from this higher number of targets on a small cohort of samples to identify the targets that give you the clinical utility. Then, ideally, move on only with very few or the least number of targets on a big cohort so that you can really have clinical value and validate your findings. Eventually in the future, as I mentioned during the presentation, we will want to use the data that we generate with mIF to train AI algorithms to be able to just use H&E.
Lorcan: Yes, I agree with what Angela said there. Maybe just from a digital pathology perspective, protein versus RNA, both HALO and Visiopharm software have got some great modules for the detection of the RNA and protein signals, be it sort of a spot signal or a clump of spots. These signals or stains are captured in different channels, then the signal can be co-localized and detected. Certainly with the image analysis available we are able to do that.
From a target perspective with image analysis, the number isn’t really the issue. From a practical sense though, you may need to think about when you get up to something like 100 targets, how you will develop your algorithm or how you’ll look at phenotypes in different cells. When you’ve got so many different markers, it becomes really quite challenging. Angela is right, the higher numbers of targets are usually more associated with the earlier discovery studies. There you’re doing “a look and see” to determine what’s coming out of interest that you may not know of. Then, as you gain confidence in certain biomarker profiles as part of a project, you may start to reduce your panel to be able to build more robustly that dataset around particular cell types or sub-cell types. So yes, from an image analysis perspective, these are doable.
Something else to think about with 100-plex studies is to make sure you have confidence in your section that you’re generating. Is it representative of the tissue and is it reproducible, and so forth. It’s certainly a dynamic and interesting area when we discuss the level of plex. As we move towards the clinic, I think getting more focus on that and triaging down to something that can be more reproducible is key.
If you have any questions, or would like more information on some of the topics discussed during this Q&A session, please look through our scientific content available in our resource center, https://ultivue.com/resource-center
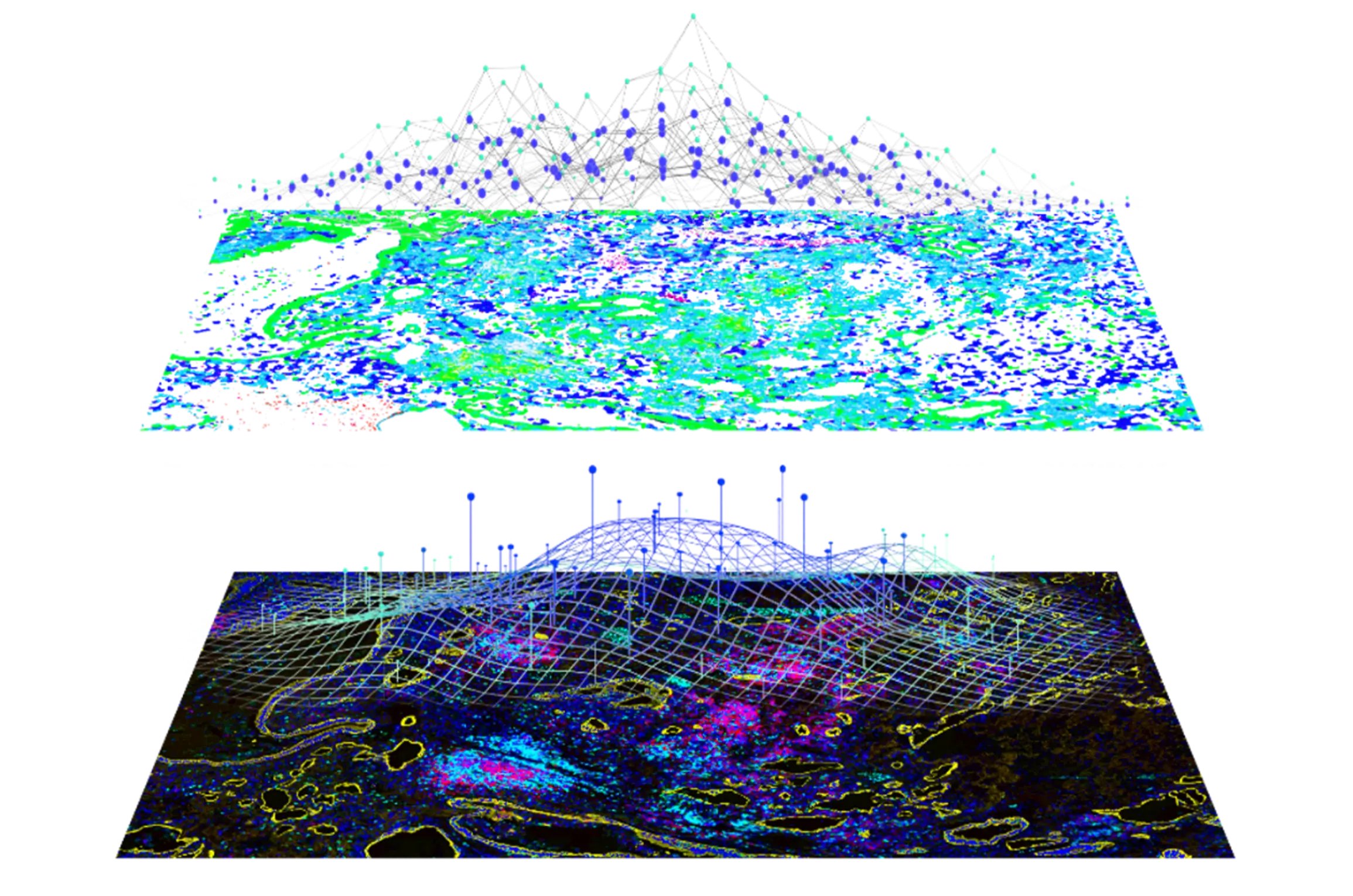
hafadmin Categories: Uncategorized Tags: immunofluorescence, spatial biology, tumor microenvironment 5383 Back in the Saddle at the AACRIn her opening remarks for the conference, Margaret Foti, CEO of the AACR, noted that “despite the challenges, this is an incredibly exciting, innovative, and hopeful time in cancer research. As reflected in the theme of this year’s meeting, decoding cancer complexity, integrating science, transforming patient outcomes, the pioneering strides you and your colleagues are making across the spectrum of cancer science are driving transformative progress against the disease at an exhilarating pace.” As we think about some of the strategies to deconvolute the complexities of cancer, especially within the tumor environment, one area in particular that dominated talks and posters this year was some of the recent advances in spatial technologies and multiplex approaches, from single to multiple biomarker assessment.
As outlined in his AACR 2022 summary, Colin Enderlein, DeciBio, observed that 2022 was “shaping up to be a transformational year for Multiplex Tissue Analysis (MTA) and Digital Pathology (DP), with ~20 clinical and marketing partnerships already announced these past ~4 months, and >2X the volume of spatial-omic activity seen at AACR vs prior years” (DeciBio). Indeed, a timely opinion piece from Nature Methods, published ahead of the AACR but referencing several areas of work highlighted specifically at the conference, had this to say about the use of multiplexed immunofluorescence (mIF); “we expect that advances in probes, barcoding strategies, affinity reagents, multiplexed detection, microscope sensitivity and microscope throughput will continue to move highly multiplexed tissue imaging forward in important ways. We also think improved methods for integrating multiplexed imaging data with other omics technologies will be crucial to the next phases of technological advancement. Finally, improved algorithmic and software tools for viewing and analyzing highly multiplexed and multi-modal omics data will also be needed to make the most of these advances.” I couldn’t agree more.
Ahead of the main conference, on Friday, April 8, in collaboration with Hanson Wade, Ultivue hosted our 2nd annual Biomarker Insights Summit, a day-long symposium designed to promote thought leadership and engage those working towards better understanding, diagnosis, and treatment of cancer via immuno-oncology approaches. Our esteemed speakers and panelists shared their efforts and lessons learned to better inform therapeutic approaches, including how innovative multiplex and digital pathology insights can provide benefit to clinical trials. The lively morning session covered a variety of “spatial phenomics” techniques to better understand tumor diversity, and why a greater understanding of the immune repertoire within the tumor microenvironment will be necessary to better stratify patients. Importantly, while our panel discussion centered on how we strategically think beyond the clinical utility of PD-L1, it’s clear that there remain differences between views of the pathologists vs. oncologists around the most optimal approach to clinical use. A networking lunch was extremely valuable for candid discussions, and it was great to see such enthusiasm for integration of spatial analysis into translational programs, including the variety of workflows available. The afternoon session continued with many details of implementing mIF, including assay reproducibility and validation, image analysis methods and preferred parameters to describe tumor and immune cells within a given tissue. The dynamic panel discussion touched on sources of ground truth for training AI models, a concern given the inter-pathologist variation in tumor assessments. With additional talks from our co-marketing partners at Aignostics and Paige, it was encouraging to see the emergence of cohesive spatial workflows that combine the power of mIF and AI development, a topic we look forward to hearing more about in the future.
Artificial intelligence (AI), which holds great potential to improve cancer diagnosis, prognosis, and prediction of response to therapy, was featured widely at AACR 2022. Dr. Su-In Lee, University of Washington, in a session on AI models discussed how explainable AI (XAI) can be used to predict clinical outcomes. She showed how datasets from patient tumor cohorts that include gene expression levels and the effects of different combinations of drugs on their biological targets can be used to train a machine learning model that can predict how synergistic untested combinations of drugs might act in different patients. “XAI can help us make new biological discoveries from data and may inform clinical decisions, and even open new research directions in biomedicine,” she said. Many speakers in the session, however, cautioned that while promising, such techniques have not yet become standard practice because of a lack of interpretability and transferability in translational medicine.
In keeping with the theme of integrating biomarker discovery with digital pathology, an important educational session from Drs. David Rimm, Janis Taube, and Tomas Kirchhoff discussed the importance of predictive biomarkers in the adjuvant immunotherapy setting, especially biomarkers to determine which patients need additional therapy and who can stop treatment. It was clear that the current crop of tissue-based biomarkers of immune checkpoint inhibitor (ICI) outcomes have severe limitations in precision medicine applications, owing to their woefully inadequate predictive power, high assessment costs, and difficulties with specimen availability. However, as noted by Dr. Taube, analysis of the resected specimens that have already been under therapeutic pressure can provide valuable information on how well the immunotherapy has worked in that patient, as well as revealing mechanisms of recurrence and resistance.
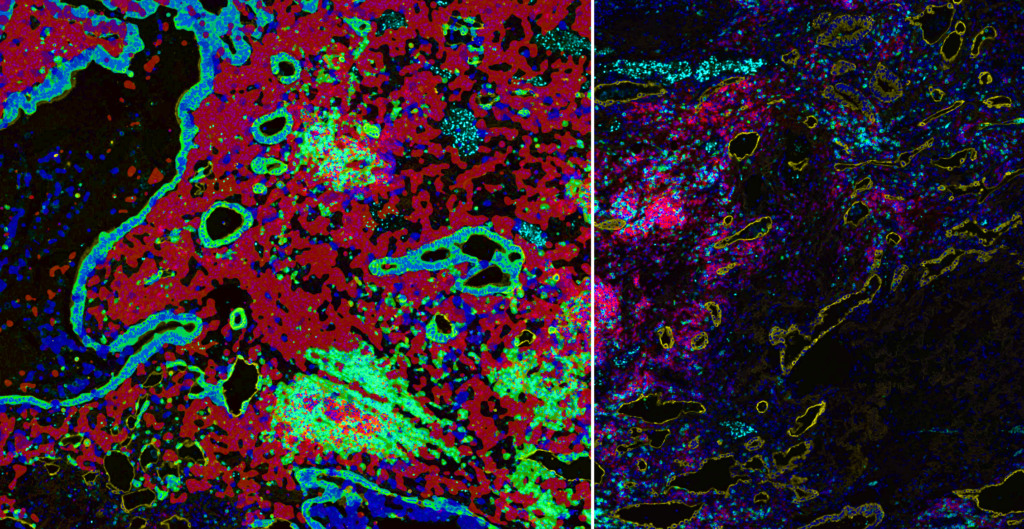
Ultivue presented several posters during the conference sessions, including a pre-optimized protocol for mIF staining on mouse tissue that provides a new way to investigate T-cell phenotypes in preclinical syngeneic or genetically modified mouse model tissues. Another poster featured our new flexible mIF assays (FlexVUE™ panels) for discerning relevant distributions of infiltrating immune cells in tumors coupled with UltiStacker® software for producing detailed spatial characterizations of specific cell phenotypes. Many scientists who stopped by our posters commented on, “how beautiful our images are.” A collaborative poster between Ultivue, Fluidigm (recently rebranded as Standard Bio Tools), and Visiopharm combined each company’s expertise to create a workflow that can unravel the complexity of the tumor microenvironment in pancreatic adenocarcinoma. Our newest workflow demonstrated co-detection of both protein and RNA on a single tissue section, and we look forward to sharing a white paper on this exciting application in the next few weeks.
Overall, despite the long days and my inappropriate footwear (I should have known that a conference was not the time to rock new heels), it was a fantastic educational meeting, and so great to hear from so many peers and experts at the forefront of cancer research. It was great to talk to the many vendors working on their unique solutions in the field of spatial biology, and especially to the scientists using these methods to unravel the complexity of cancer. It is becoming increasingly clear that the integration of “spatial phenomics” into translational efforts in the lab and the clinic is poised to deliver a much-needed promise to patients of better outcomes. However, a key takeaway is that the fight is not over yet; we must work better together!
Eva
Categories: Uncategorized Tags: Point of VUE
3042
Better Laid Plans of Mice and Men
Research in the field of humanized mice began in the late 1980s, a few years after the discovery of mice with severe combined immunodeficiency (SCID) resulting from a spontaneous mutation, specifically, Prkdcscid, (protein kinase, DNA activated, catalytic polypeptide; severe combined immunodeficiency allele) identified in a colony of C.B-17 mice. This functional inactivation then led to defective DNA repair and repair-dependent somatic V(D)J recombination of B and T cell receptor-encoding genes, resulting in the absence of mature B and T lymphocytes. Taking advantage of the severe immunodeficiency of these animals, several groups then successfully transplanted human PBMCs (peripheral blood mononuclear cells), human bone marrow cells, human fetal tissues, or human HSPCs (hematopoietic stem cells) into SCID or equivalent recipient mice models. These humanized mice can accept the xenografted elements of the human immune system and as a result, the have an immune system that is part mouse part human. Next, by xenografting cancer cell lines or patient tumor explants into such mice, the effect of an intervention such as a drug treatment on the xenograft in the context of an intact immune system can be investigated. Thus, establishment of cell-line-derived xenograft (CDX) and patient-derived xenograft (PDX) into humanized mouse models has been a remarkable stride for facilitating diverse applications in the exploration of cancer pathogenesis, and the evaluation of therapeutic effects.
While CDX models are less time-consuming to generate, the in vitro culture step before engraftment typically leads to substantial loss of primary tumor features. PDX mice on the other hand, largely retain the key characteristics of the patient’s tumors, including histological features, genomic signatures, and the heterogeneity of cells in a tumor mass, particularly the tumor immune microenvironment (TiME), visualized using multiplexed immunofluorescence (mIF) techniques. Therefore, these mouse models can potentially serve as a more accurate platform for predicting therapeutic outcomes.
An area of active research is resistance mechanisms to immune checkpoint blockade therapy, and to identify therapeutic combination strategies to enhance effectiveness for treatment in these tumor types. For example, a recent publication (2) explored why most hepatocellular carcinoma (HCC) patients currently respond poorly to anti-PD1 therapy.
Hepatocellular carcinoma (HCC) remains one of the most prevalent and life-threatening malignancies globally. Unfortunately, over 60% of HCC patients are diagnosed at advanced stages, and therefore cannot undergo curative surgery. While ICB (immune checkpoint blockade) therapies, especially with antibodies against the PD1/PD-L1 signaling axis, have made impressive breakthroughs in cancer treatment, clinical trials of HCC patients have not shown statistically significant improvements owing to primary or acquired anti-PD1 resistance. The group noted that the zinc finger protein, ZFP64 was frequently upregulated in HCC tissues of anti-PD1 resistant patients, with additional experiments indicating that a PKCα/ZFP64/CSF1 axis was critical for triggering immune evasion and anti-PD1 tolerance. Of interest, Gö6976, an inhibitor of PKCα, when introduced to both PDX and orthotopic xenograft tumor models, significantly suppressed tumor progression and altered the TiME via the PKCα/ZFP64/CSF1 axis in HCC, as measured using mIF techniques. Importantly, the group presented extensive evidence that the combined treatment of Gö6976 with anti-PD1 could synergistically improve the survival of tumor-bearing PDX mice, especially in the subset overexpressing ZFP64.
With the accumulating evidence from many publications (3,4), the use today of PDX and “better” improved humanized mouse model designs, as well as updated methods to visualize cell and spatial contexture, have become highly effective in predicting the efficacy of both conventional and novel anti-cancer therapeutics. Indeed, ongoing areas of research now afford “co-clinical trials,” in which pre-clinical investigations in vivo and clinical trials can be performed in parallel or sequentially to assess drug efficacy in mice (PDX) and men (patients).
Historically, detection of protein targets from different species in the same tissue section was difficult due to dependence on species-specific secondary antibodies (e.g. goat anti mouse secondary antibody to detect an mouse antibody made against a human protein). Ultivue’s direct antibody labeling technology eliminates detection barriers due to species, allowing rapid creation of multiplex reagents against targets from multiple species in the same multiplex panel. For more information on how to incorporate multiplexed immunofluorescence from your PDX or humanized mouse model and derive valuable spatial information from the tumor microenvironment, please visit www.ultivue.com.
hafadmin Categories: Uncategorized Tags: Point of VUE Comments 788 The Much-Welcomed Return of In-Person ConferencesI was therefore thrilled to attend my first in-person event in 2022, in Brooklyn, New York: the 8th annual Immuno-Oncology 360 event, #IO360NY. The enthusiasm and excitement of researchers finally gathering to exchange scientific ideas and discourse was evident; we all missed the real, human connection to our peers. Scheduled over 3 days, the comprehensive program convenes stakeholders spanning the science, clinical, and business communities to report on the latest data-driven advancements in Immuno-Oncology in a wide variety of tumor types. It was a packed program, and for the sake of this summary, I’ll instead review my own highlights, but please feel free peruse the agenda herein, https://theconferenceforum.org/conferences/immuno-oncology-360/overview/.
Day one began with the keynote address by 2019 Nobel laureate Dr. Gregg Semenza, Johns Hopkins, discussing mechanisms of tumor immune evasion mediated by the hypoxia inducible factor (HIF) system and the impact targeting HIFs has had on cancer immunotherapeutic strategies. His discovery of HIFs has now been recognized as having far-reaching implications for understanding and treating a variety of conditions, such as cancer and ischemic cardiovascular disease, in which hypoxia plays an important role in disease pathogenesis. Dr. Semenza showcased elegant, as yet unpublished work from his lab identifying several small molecule candidate drugs in a screening assay that potently inhibit HIF-1 and block cancer progression in mouse models of hepatocellular carcinoma yet avoid anemia as an on-target toxicity associated with HIF therapies to date.
Day two showcased highlights in imaging, operations, partnering, and biomarkers in the I/O field, with the annual top 10 I/O recommendations and what’s next on the IO radar from CITI analyst, Dr. Andrew Baum. With the wealth of public information, its often hard to keep up with the latest developments in the field, so I find his talks both insightful and very impactful in reviewing the past years “winners” and “losers” in the I/O drug development race as well as dynamics affecting the US biotechnology sector. I think many of us await with bated breath the outcome of some of phase 3 TIGIT data due this summer. The list of Top 10 drugs/therapy strategies to watch out for in 2023 didn’t change dramatically from 2022, top to bottom: TIGIT; ADC’s; ILT4/LILR2b; TGF-beta; Bi-specifics; IL2/15; DDR’s/PARP; TCR/CAR-T; oncolytic viruses, and rounding out the list, targeted CD28 therapies.
A highlight was the annual “great cancer immunotherapy debate” featuring Drs. Robert Valamehr from Fate Therapeutics vs. Kristen Hege from Bristol Myers Squibb on the merits of different chimeric antigen receptor therapy (CARs) platforms, with newcomers to the fray natural killer (NK-)-CARs being challenged by T-cell-CARs of which there are now 6 FDA approved products. Dr. Hege immediately launched into the undisputed success of CAR-T therapies, and why only T cells that are capable of directed cell killing; her quote that “this cell type is the culmination of many years of evolution to become powerful killing machines” isa strong argument indeed. Dr. Valamehr’s response was swift and to the point: NK cells instead have spontaneous cytotoxic activity and can generate target cell death independent of the tumor target antigen, while T lymphocytes only kill their targets by a CAR-target specific mechanism that is susceptible to resistance mechanisms. Dr. Hege pointed out that today, with hundreds of clinical trials in progress, CAR-T cells have shown astonishing results in the treatment of relapsed or refractory hematological malignancies, but she acknowledged the challenge in solid tumors where efficacy and toxic side effects were still issues, a concern that Dr. Valamehr seized upon in his rebuttal arguments. Ultimately, concluding her comments focused on cytoxicity, Dr. Hege argued that with the wealth of information now available, “we’ve learnt a lot about the side effects associated with CAR-T and can predict these, most side effects are low grade and reversible.” Preclinical evidence thus far suggests NK-CARs are indeed less toxic, and her final comment was that patients want an effective proven therapy over a toxic one. The field of CAR-cellular therapies is still maturing, but preclinical and clinical studies have already shown remarkable results, and both researchers agreed that much of the data is profoundly promising, leading to the development of approved personalized therapeutic options in the future. I, for one, look forward to hearing more from these worthy opponents in future meetings.
Several of my esteemed colleagues at Ultivue were also in attendance at the meeting, our own VP Medical Director, Keith Wharton delivered a wonderful summary outlining the need for multiplexed tools in the era of cancer immunotherapeutics and the wealth of information that can be achieved from single whole slide imaging of tumor samples to better inform translational research efforts and clinical practice in Immunotherapy. If you missed our booth and/or would like more information on how our tissue-based solutions can help guide your research, please visit www.ultivue.com; specifically, our pre-optimized panels that are currently available www.ultivue.com/products/
It was overall a welcomed return to in-person meetings, having the opportunity to candidly discuss and follow up with each of the speakers in their respective fields of expertise. Whilst I wholly recognize the benefits to democratizing science through virtual meetings, attending in person is key to networking, collaborating, sharing information, especially if it is over coffee or even a cocktail!
hafadmin Categories: Uncategorized Tags: Point of VUE Comments 787 The Crossroads Between Immuno-Oncology and Digital PathologyThe podcast began with a review of Ultivue’s innovative InSituPlex® staining technology and service offerings enabling key insights into the tumor microenvironment as well as what makes these workflows so unique, by outlining the differences between single marker IHC approaches and other techniques such as FISH and addressing the importance of standardization and reproducibility.
One of the exciting areas of opportunity for integrating digital pathology is the journey from biomarker/drug discovery to drug approval to implementation in clinical practice and then, of course, one arena for future developments in diagnostics is a multiplexing-based companion diagnostic. Dr. Wharton noted that while “I don’t think the field is there quite yet”, we’re instead “at the stage where we’re using the technology to help our customers get a better understanding into simply what they’re seeing in tissue.” Dr. Wharton pointed out that while digital pathology studies are often done on retrospective cohorts, large tissue collections with outcome data present an opportunity to generate and test hypotheses leading to deeper clinical insights.
The podcast finally reviewed other topical areas such as the role of deep learning, AI and integration of more traditional methods such as H&E and ultimately speculated on the possibility of digital pathology as the platform of choice for an integrated clinical diagnostic that incorporates molecular data (e.g. DNA hybridization), multiplexed protein detection, and tissue features derived from methods such as H&E staining. The opportunity that these evolving innovative methods will bring, especially to the arena of immunotherapeutics, will mark significant changes in the field in the coming years.
There’s lots more, to listen to the full podcast:
Due to their heterogeneous nature, tumor tissues vary considerably in their microenvironment, and the existence of a variety of cell types can dramatically influence the ability of the immune system to infiltrate and attack tumor cells. analysis can be used to characterize the immune cell repertoire, identify various cell populations in the microenvironment. Tumor-associated macrophages (TAMs) represent one of the main tumor-infiltrating immune cell types addressed in the tumor microenvironment and studies have shown that this TAM population is in a state of constant transition between two forms referred to as M1 and M2 types. M1-type macrophages have anti-tumor effects, which can distinguish tumor cells from normal cells. By identifying tumor cells, expressing e.g. nitric oxide synthase (iNOS) and ultimately killing tumor cells, studies have found that M1 type macrophages exhibit different effects on killing tumor cells. These macrophages can also present tumor-specific antigens to T cells and help in the anti-tumor immunity. Conversely, M2 has the function of removing debris, promoting angiogenesis, tissue reconstruction and injury repair, as well as promoting tumorigenesis and development. The majority of TAMs are of the M2 phenotype (e.g. expressing CD163) and have poor antigen presentation capacity and can suppress the T cell response, importantly therefore the need for selective M2-to-M1 macrophage repolarization has drawn attention for effecting immunosuppression and improving antitumor responses. Recently, a variety of therapeutic agents (e.g., monoclonal antibodies, small molecular inhibitors, and nanoparticles) have been extensively explored for M2-to-M1 macrophage repolarization.
Using a cyclic RGD peptide functionalized and manganese doped eumelanin-like nanocomposites (RMnMels) Liu et. al., 2022 reported a novel combined hyperthermia-immunotherapy against PC3 prostate cancer in mouse models demonstrating that RMnMels could successfully promote M2-to-M1 macrophage repolarization via scavenging multiple reactive oxygen species and remodeling the immunosuppressive tumor microenvironment. Specifically, following near-infrared light irradiation, RMnMels-mediated thermal ablation could destroy the tumor cells directly, but also in part using a tissue immunofluorescence assay addressing CD163 and iNOS, RMnMels could elicit the release of damage associated molecular patterns and tumor-associated antigens, provoking robust tumor immunogenicity and strong antitumor immune responses. I’ll be following with interest the future developments of RMnMels and other therapeutic nanoplatforms for immunomodulation and enhanced antitumor immune responses.
Advances in multiplexed immunofluorescence techniques have helped tremendously to visualize biologically and prognostically relevant macrophage subpopulations in the tumor microenvironment from FFPE sections. If we now think back to Hitchcock’s approach for success as simplicity in the story and guiding with relevant information, Ultivue’s InSituPlex® multiplex immunofluorescent (mIF) technology embodies these sentiments by enabling a streamlined biomarker detection and tissue analysis. The workflow begins by incubating a tissue slide with a mixture of barcoded antibodies for multiplex target labeling. Bound antibody barcodes are then amplified to increase the sensitivity of complimentary fluorescent probe hybridization. Bound probes are then imaged to provide a view of targeted cells like macrophages populations and their cellular interactions within a spatially preserved tumor microenvironment. Importantly researchers benefit from the simplified workflow and availability of Ultivue’s flexible options for pre-optimized off-the-shelf panels or custom panels that include up to 8 relevant application focused targets e.g., a TAM panel.
While the complexities of the tumor microenvironment still remain an area for great discovery, in immunotherapy research perhaps focus on the murderous M1 macrophages and their sidekicks may be the hero ending we’re all looking for.
Contact Ultivue today to see how InSituPlex mIF technology can drive discovery in your tissue biology application.
hafadmin Categories: Uncategorized Tags: Point of VUE Comments 790 It’s TIGIT TiMEIdentified over 10 years ago as a promising emerging immune checkpoint target, T cell immunoreceptor with Ig and ITIM domains, better known as TIGIT, has been the focus of recent scientific headlines and represented in over 60 clinical trials as of December 2021. Why the hype?
Expressed on multiple types of immune cells, including Tregs, activated T cells, and NK cells, TIGIT indirectly suppresses T-cell activation and together with its main ligand, CD155 can also contribute to local suppression of immune-surveillance. Predictably then, TIGIT expression is associated with advanced disease and poor survival outcomes and increased TIGIT expression after treatment is further associated with disease recurrence. Anti-TIGIT therapy is therefore key and presumed to stimulate immune function and enhance the activity of both T cells and NK cells so it was somewhat surprising that many studies using single TIGIT blockade revealed limited anti-tumor efficacy.
TIGIT targeting instead is likely to be most efficient when combined with other immunotherapies. Already various pre-clinical and early phase clinical studies indicate that blockade of TIGIT together with the PD-1/PD-L1 pathway leads to tumor rejection in a variety of indications, perhaps through a mechanism of tumor antigen-specific CD8+ T cell expansion.
Evidence to date looks promising and recent work (Wen et. al., 2021) analyzed the expression patterns of the TIGIT and its value of prognostic prediction among 33 types of cancers based on the data collected from The Cancer Genome Atlas (TCGA) and the Genotype-Tissue Expression projects (GTEx) noting correlations of TIGIT with pathological stages, tumor-infiltrating immune, signatures of T cells subtypes, immune checkpoint genes and the degree of Estimation of STromal and Immune cells in MAlignant Tumor tissues using the Expression data (ESTIMATE).
Clearly TIGIT expression varies between tissue compartments and cell types in normal and tumor conditions underscoring the importance and need of a detailed in situ immunophenotyping analysis of patient tissue samples to address the balance of immune inhibitory and stimulating markers within the tumor immune microenvironment (TiME).
In the end fundamentally addressing a potential immunosuppressive landscape and identifying TIGIT interactions may provide not only the valuable information for which patient will benefit but also the design of more effective treatment options in cancer.
Want to explore the expression of TIGIT and other markers in your tissues? Check out some of our newest panels enabling a detailed interrogation of the tumor microenvironment associated with specific cancer types.
For more information on any of our products and pre-optimized panels visit https://ultivue.com/panels/.
hafadmin Categories: Uncategorized Tags: Point of VUE Comments 784 TiME for a New Vue of the Tumor LandscapeHave you ever stood so close to a painting that you could see the brush strokes left behind on the canvas? I often marvel at the level of detail in a beautiful landscape painting. I imagine the artist applying layer by layer of paint, adjusting the colors, and blending to make sure the color and lighting are just right. If you stand too close to the painting for too long observing all the details, you begin to lose sight of what those brush strokes have created. Only when you step back to take in the scene can you have a full understanding and appreciation for how the individual elements come together to create a work of art.
I am reminded of this when I think about all the thousands of experiments performed by scientists to define the complex biological interactions occurring within the tumor immune microenvironment (TiME), a landscape filled with a diverse population of tumor-infiltrating lymphocytes (TILs), tumor cells, protein biomarkers, inflammatory markers, and more that influence disease progression and response to cancer therapy.
To date, much of what has been learned about the TiME has come from the use of immunohistochemistry (IHC), a standard method used by pathologists as a screening tool in immuno-oncology. IHC has helped identify biomarkers and immune cell types within the TiME, but information has been limited by labor-intensive protocols that yield single data points. IHC methods are not sufficient for generating a comprehensive and interactive picture of the TiME landscape – only layer upon layer of superimposed data with reduced spatial resolution. Newer technological approaches, such as multiplex immunofluorescence (mIF), provide greater resolution, better use of precious sample, and unparalleled insight into spatial cellular arrangement within the tumor. Technologies like mIF can paint a clearer picture of a patient’s immune status and disease state and corollary provide more information to promote successful immunotherapy.
As we learn more, we recognize that much more remains to be understood regarding the complexity of the TiME and that advanced tools are needed for better insight. A recent publication by Jianghua Wu, et al1describes the validation of mIF and its comparison to IHC for the analysis of programmed death-ligand 1 (PD-L1) expression and immune cell profiles within non-small cell lung cancer (NSCLC). Current clinical stratification for NSCLC immunotherapy requires positive measurement of tumor cell surface PD-L1 expression and a derived tumor proportion score (TPS). A challenge to assessing PD-L1 and TPS arises inthat PD-L1 is also expressed on some immune cell subtypes leading to a complex staining pattern within the tissue that makes clinical interpretation difficult.
This study was conducted to compare the cell density of PD-L1 expression and immune cells in NSCLC tissues stained by IHC and InSituPlex® DNA-barcoded mIF. Stained tissues were assessed using digital image analysis (DIA) to validate the cell density of PD-L1 and immune cells. A TPS generated from combining mIF and DIA was compared with manual PD-L1 calculation by pathologists using IHC. Findings from the study demonstrated a high correlation in immune cell densities and TPS between IHC and mIF. Greater detail and insights into cellular identity and biomarker expression were achieved using mIF, whereby simultaneous detection of both PD-L1+ and cytokeratin epithelial cell marker+ (CK+) enabled differentiation of PD-L1+ tumor cells from PD-L1+ T cells and PD-L1+ macrophages. Detection of PD-L1+CK+ and CK+ cells permitted calculation of a quantitative TPS. Studies also showed that the calculation of TPS using a combination of mIF and DIA compared favorably to TPS calculated using IHC and pathologist review.
Spatial insight into distances between tumor cells and specific immune cell types within a tissue section were enabled using mIF and digital imaging. In this study, distances were further between PD-L1+ tumor cells and immune cells than between PD-L1- tumor cells and immune cells. Data also showed that T cells were closer to PD-L1- tumor cells. In a single experiment, mIF permitted a clear view of the phenotypic complexity and cellular arrangement within NSCLC tissue.
The Wu, et al. study demonstrated that InSituPlex DNA-barcoded mIF is comparable with IHC methods for the quantification of tumor and immune markers and superior in its ability to discern target localization. Further studies are needed to correlate singleplex IHC assays to multiplex assays.
Ultivue’s InSituPlex multiplex immunofluorescence (mIF) technology outperforms IHC for simultaneous multi-target detection in spatially preserved tissues. Investigators will benefit from simplified workflows and availability of pre-optimized panels or custom assay panels with up to 8 targets where one can select >70 immune-relevant targets or incorporate your own novel target. Panels are compatible with most scanning instruments and digital imaging software. Importantly, the use of multiplex biomarker characterization in a spatially preserved context will provide greater depth of analysis and advance both an understanding of tumor biology and effectiveness of immunotherapy.
Our view of tumor biology has been built using IHC, but to paint a clearer picture of the phenotypic complexities within the TiME new tools are needed. The use of mIF will provide greater resolution and better use of precious samples to provide greater insight and advance targeted immunotherapy.
hafadmin Categories: Uncategorized Tags: Point of VUE Comments 783 A Brief History of TiMEStephen Paget considered the founding father of TiME laid the foundations of this research area by formulating the seed and soil theory postulating that metastasis of a particular type of cancer (“the seed”) often metastasizes to certain sites (“the soil”) based on the similarity of the original and secondary tumor sites. Numerous studies in the 1970’s and 1980’s elaborated on the immune and angiogenic factors involved in this interplay of the tumor and its environment by characterizing the functions of cellular and humoral immune components. These studies established that these immune cells including T cells, B cells, NK cells and macrophages had the capacity to infiltrate solid tumors in humans and in animals (reviewed in Witz, 2009). Other early studies from Judah Folkman’s lab appreciated that tumor proliferation was dependent upon blood supply and that the interactions of tumor and endothelial cells initiated and drove this process. Angiogenic factors were then identified in various types of tumors and the possibility was raised that inhibiting such factors or their interaction with endothelial cells could perhaps be of clinical benefit to cancer patients (reviewed by Folkman J, 1972). Subsequent work by others also highlighted the interactions between the stroma and tumor cells. The stroma consists of the extracellular matrix (ECM), which is composed of proteoglycans, hyaluronic acid, and fibrous proteins such as collagen, fibronectin, and laminin; growth factors, chemokines, cytokines, antibodies, and metabolites; and mesenchymal supporting cells (e.g., fibroblasts and adipocytes), cells of the vascular system, and additional cells of the immune system. As tumors develop, the stroma also evolves.
It was a seminal paper 30 years ago that really changed the landscape of how we view the role of immune cells in the tumor microenvironment. van der Bruggen and colleagues first reported the existence of a human tumor antigen recognized by T-cells. They were able to clone the melanoma antigen-encoding gene (MAGE), which encodes an antigen recognized by cytotoxic T-cells, providing not only evidence that the immune system was capable of seeking and destroying tumor cells but also provided the first identification of a molecular target, one that is actively used clinically for advanced melanoma.
Today, the complexity and functional contribution of the tumor microenvironment in cancer progression much like our knowledge of the universe continues to expand at the cellular, organ and systemic level. This complexity is observed within not just the variety of cells involved, but also includes metabolism as a form of communication, aging and obesity as microenvironmental factors at the tissue and systemic levels, and the significance of gut microbiota. It is now appreciated that the composition of the tumor microenvironment plays a significant role not just in disease progression, but also in response to therapy, invasion, and metastasis or conversely, restraint of growth for many tumor types.
Recent work by Grunwald et. al., 2021 have discovered additional complexity to this vast cancer cosmos, with the identification of ‘‘subTMEs,’’ histologically definable tissue states anchored in fibroblast plasticity, with regional relationships to tumor immunity, subtypes, differentiation, and treatment response. They noted that “reactive’’ subTMEs, functionally coordinated fibroblast communities were immune hot and inhabited by aggressive tumor cell phenotypes yet appeared more chemo-sensitive. The matrix-rich ‘‘deserted’’ subTMEs instead harbored fewer activated fibroblasts and tumor-suppressive features but were markedly chemoprotective and enriched upon chemotherapy. Its clear from this study and others that we are still only just beginning to explore these new dimensions addressing the tumor-stroma-immune interplay in tumor progression, patient-specific stromal heterogeneity and how this is linked to clinical outcomes.
Want to explore this universe in your tissues? Check out some of our newest panels enabling a detailed interrogation of the tumor microenvironment associated with specific cancer types.
hafadmin Categories: Uncategorized Tags: Point of VUE Comments 782 The Path(ology) Not TakenThe practice of anatomic pathology today rests on a century and a half legacy of histopathology – the changes in cells and tissues in various disease states as seen in a microscope. Virchow and other giants of the 19th century recognized the importance of these changes, and many of their concepts endure. Visual interpretation of thinly sliced tissue sections, embedded in candle wax and stained blue and pink with the textile dyes hematoxylin and eosin, remains the “gold standard” for diagnosis of many diseases.
I was fortunate in my first job out of college to work with a pathologist, studying changes in heart tissue following our attempts to reverse abnormal heart rhythms. I remember with awe the fine, delicate detail revealed in tissue sections, as well as the power of careful observation. I was struck by the diversity of cells – each with the same DNA, yet each with a distinct position, shape, and role in the muscle and its healing process. How did each cell know who it was, where it was, how to behave, and when to stop or die?
Well, I did become a pathologist but quickly recognized that pathology was largely correlative, full of conjecture, and (at that time) ultimately unable to address these questions. My journey to answer these questions led me over two decades to molecular and developmental biology, studying mostly fruit flies and mice. Why? We now know that cells adopt different identities using combinations of transcription factors and talk to each other with signaling modules, using a mostly ancient and relatively small “toolkit” of proteins that unite not only all of us as humans, but all of the earth’s creatures, including flies and mice.
Times have changed. Anatomic pathology is at the tipping point of a revolution fueled by advances in biology, technology, digital and computational pathology, and artificial intelligence. These questions about cells can’t be addressed using current immunohistochemical techniques or bulk tissue sequencing, but are amenable to tissue multiplex analyte detection. In particular, accurate characterization of each cell in tissue biopsy, especially with respect to the “tumor immune microenvironment” (TIME), is increasingly important to characterize cancer tissues and predict response to new therapies. Our innovative InSituPlex staining technology and services offerings can provide key insights into these and other questions important for research and drug development. Finally, with Ultivue colleagues we’ve summarized our perspectives and view of the future in a peer-reviewed open access article available at the link below. We welcome your feedback and look forward to using InSituPlex to help solve your tissue mysteries.
Click here to access the Frontiers review article hafadmin Categories: Uncategorized Tags: Point of VUE Comments 781 Don’t Knock It TIL You’ve Tried ItMy name is Kirsty Maclean Ph.D. and I’m the Senior Director of Scientific Marketing at Ultivue. Originally from Scotland, like so many other Europeans I moved to the US for my post-doctoral studies. The late 1990s was a pivotal time in science: novel methods of gene manipulation for knock out/knock-in mouse models of cancer were being explored, along with game-changing tools like microarrays to measure transcript expression. However, the human genome published in 2001 changed the face of biology and rapidly catalyzed a transformation of scientific progress and medicine. I’ve always been curious, with a need to be on the cutting edge of scientific innovation, so after a successful academic career I moved to the rapidly evolving world of biotech. A 15-year journey in this space ultimately led me to Ultivue, their novel InSituPlex® assay, and following advances in tissue multiplexing.
Immunohistochemistry (IHC) has come a long way since my post-doc days in that it required tedious, labor-intensive protocols and -to be honest -left you with limited information beyond your single marker of interest (mine was p53!). Today, technology that integrates multiplex marker detection with single-cell resolution and retaining tissue context provides new insights into cellular composition, cellular functions, and cell-cell interactions.
Tumor infiltrating lymphocytes (TILs) are usually assessed by pathologists in tumor biopsies because they can have prognostic value for the patient. They are even more important in cancer immunotherapy, because most therapies try to activate TILs to kill the tumor. But when you see TILs in a tissue slide stained with hematoxylin and eosin (H&E), they all look alike! IHC labels one marker at a time; and the number and density of TILs is typically estimated by eye.
A new study using two-marker multiplexed immunohistochemistry (mIHC) of CD4, CD8, and FOXP3 expressionby digital image analysis investigated the distribution of T-lymphocyte subsets in hereditary breast cancer (Jørgensen et. al., 2021). Notably, they demonstrate that a high percentage of CD4-, CD8-or FOXP3-positive TILs was associated with lower mortality, and the presence of CD8-positive TILs – the subset that can help the body kill tumor cells – was related with disease-free survival.
This is one of a growing number of studies we plan to highlight that demonstrates single-marker IHC is inadequate to address the many multi-faceted problems facing immunotherapy. Picking multiple biomarkers, and critically the right biomarkers to identify the key cell types – while utilizing less biopsy material -may provide better answers for physicians and their patient.
With that in mind, our InSituPlex technology enables whole tissue slide labeling of these important T cell subsets as well as detailed exploration of the tumor microenvironment -all while preserving tissue morphology to enable same slide traditional H&E staining (compared to other technologies in excellent reviews by Tan et. al, 2020 & McGinnis et al., 2021). We provide flexible options, including optimized off the shelf panels and up to 8-plex custom assay development (from our menu of >70 immune-relevant targets or your own targets) so scientists can realize the benefits of comprehensive biomarker assessment, co-localization, and compartmentalization to address their hypotheses, and we hope ultimately to help develop and predict responses to therapy.
I often think back to my post-doc days, where just a single experiment of the many replicates needed to convince yourself (or journal reviewers!) took weeks and weeks of work. Today, efficient tissue insights using multiplexed immunofluorescence can arm clinical trials to extract more advanced information from tissue biopsies, and importantly, might better predict how patients will respond to certain treatments.
For more information on any of our panels visit https://ultivue.com/products/
For more information on Ultivue services visit https://ultivue.com/assay-dev/
hafadmin Categories: Uncategorized Tags: Point of VUE CommentsYou are currently viewing a placeholder content from Facebook. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More InformationYou need to load content from reCAPTCHA to submit the form. Please note that doing so will share data with third-party providers.
More InformationYou are currently viewing a placeholder content from Hubspot Embedded Content. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More InformationYou are currently viewing a placeholder content from HubSpot. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More InformationYou are currently viewing a placeholder content from Hubspot Meetings. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More InformationYou are currently viewing a placeholder content from Instagram. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More InformationYou are currently viewing a placeholder content from X. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More Information

 Uncategorized
10026
Ultivue Announces its STARVUE™ Image Data Science Platform, Providing Researchers with an Integrated, AI-Driven Analytical Solution for Generating Spatial Insights Copy
Uncategorized
10026
Ultivue Announces its STARVUE™ Image Data Science Platform, Providing Researchers with an Integrated, AI-Driven Analytical Solution for Generating Spatial Insights Copy
